

MY HEART was breaking, but not from lost love. It was failing in a more literal sense.
In 2020, my doctor recommended that I get an echocardiogram — an ultrasound of the heart — to establish a baseline against which to monitor any changes as I aged. Though I felt perfectly fine, the image revealed that I had developed mild aortic stenosis, a narrowing of the valve that controls the flow of oxygen-rich blood from the heart's main pumping chamber (the left ventricle) into the aorta, and from there to the rest of the body.
Within a few years, the diagnosis had progressed from mild to moderate stenosis. Further change would likely be gradual, I was told. Intervention wouldn't be necessary unless and until the degeneration of the valve crossed into "severe" territory. But an echocardiogram early this year showed that the stenosis — which is caused by a buildup of calcium on the valve — was advancing much faster than expected. Suddenly, a heart operation wasn't a development to anticipate in some abstract future. According to my cardiologist, it was necessary now. I sought a second opinion, from a specialist working in a different medical practice. He reviewed the images and the data and made the same recommendation: Have this surgery.
And so, in late March, I found myself on a gurney, being prepped for the most consequential medical procedure of my life (so far).
 In the 1950s, open-heart surgery had a 50 percent mortality rate. Today it is less than 1 percent. |
Open-heart surgery is the sort of experience you tend to regard as too remote to even think about — until it's scheduled for you. But the weeks leading up to the procedure made it clear that there is nothing theoretical about what is going to take place. Over a period of about a month and a half, I had to meet with a thoracic surgeon, choose an anesthesiologist, undergo a variety of pre-surgical imaging (X-rays, CT scan, another ultrasound), submit to catheterization to map out my heart and coronary arteries, and take part in "pre-anesthesia testing" to make plans for sedation during the surgery and pain management afterward.
The surgeon presented me with consent forms in which I acknowledged the serious risks involved in the surgery. On one of the forms, he had noted in large letters that those risks included death and stroke. I asked him how often such disasters occur. About once in 200 surgeries, he told me. In the abstract, a 0.5 percent mortality risk seems reassuringly low. It seems far less so when you reflect that you might be the one. My wife certainly took little comfort in the statistics.
In truth, during the run-up to surgery my greatest dread wasn't that I would die or be left disabled. It was that I would wake up with a breathing tube down my throat. That prospect freaked me out so much that I brought it up with every doctor I encountered. They all assured me that I would be under full anesthesia during intubation and that even if the tube were still in when I regained consciousness, I would retain no memory of it.
They were wrong. It is the first thing I remember about waking up in the ICU and I remember it vividly — the sense of being about to suffocate, the restraint of being unable to speak, the panicky urge to get that thing out of my throat. Three months later, it remains a nightmarish recollection. By contrast, I have no memory at all of being wheeled into the operating room, though I know I was conscious at the time and even waved to my wife as I was wheeled past her.
The operation itself took about four hours. What I know of it comes mostly from my own research (instead of writing Arguable, I've been reading up on the history and techniques of heart surgery and watching surgical videos), the many questions I asked, and the evidence I can see in the mirror of the surgical team's precision.
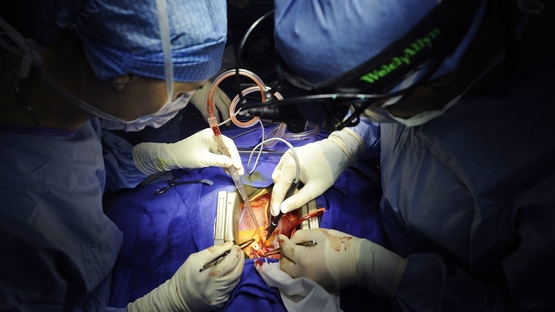
The process was at once brutal and exacting. (Warning: some graphic descriptions ahead.) After the anesthesia took hold, my chest was scrubbed and draped, leaving a rectangular area exposed. Using a scalpel, the surgeon made an 8-inch incision from just below the collarbone to the upper abdomen. The blade sliced through skin and subcutaneous fat, revealing the flat, hard bone of the underlying sternum.
An oscillating saw split the bone along the midline. A stainless steel retractor separated my rib cage and held it open, exposing the lungs and beating heart beneath. The pericardium, the sac that encases the heart, was incised and pinned back. Suction cleared the blood; cautery smoke drifted through the field; machines hummed steadily. All the while, I slept.
What followed depended less on force than on timing. Tubes and clamps redirected my blood into a cardiopulmonary bypass machine, which took over the work of oxygenating and circulating it. Then an ice-cold potassium solution, cardioplegia, was infused into the main coronary arteries. My heart slowed, relaxed, and stopped beating.
Its stillness was clinical and eerie — and essential. With the heart motionless and the blood circulating elsewhere, the surgeon could proceed to remove and replace my diseased valve.
Elie Wiesel, the late Nobel peace laureate, underwent invasive heart surgery in 2011 and afterward wrote a slim volume, "Open Heart," about the experience. "I didn't know, I couldn't know, just how complicated it is, with risks and dangers that defy imagination," he mused. "For the layman that I am, this surgery is not unlike a walk on the moon. ... I was overcome with a feeling of gratitude."
Prior to surgery, I hadn't been experiencing any severe symptoms — nothing more than a mild breathlessness when walking uphill. But if the valve wasn't removed, I learned, it would be only a matter of time before more serious symptoms appeared. At that point, the average survival without valve replacement is only 2 to 3 years. Aortic stenosis is cruel in that way — you can be relatively asymptomatic until one day you collapse. In his compelling memoir "Fragile Lives," the trailblazing British heart surgeon Stephen Westaby quotes Henry Wadsworth Longfellow: "Nothing is too late / till the tired heart shall cease to palpitate."
I had mentioned to my surgeon a couple of times that after he removed my damaged valve, I wanted to keep it as a souvenir and asked him to set it aside for me. But when I asked about it after the surgery, he told me, rather dismissively, that anything taken from the body had to be sent to the pathology lab. It annoyed me to have my simple request ignored — especially when, reading "Fragile Lives" a few weeks later, I learned that Westaby hadn't hesitated to honor a similar request from one of his patients. But considering what I owed the surgeon, I wasn't about to make a fuss over it.
In the immediate aftermath of surgery, I was full of holes. There were tubes or puncture wounds in my neck, my abdomen, my chest, my hand, and my thigh. And then there were the pacing wires — thin wires attached directly to the heart and brought out through my chest, a practice invented in the 1950s by Dr. Walt Lillehei, an American pioneer of open-heart surgery. They allow doctors to pace the heartbeat externally if its rhythm falters. Mine were never needed, thankfully, and were pulled out just before my discharge. The removal was surprisingly painless, but the very idea that I had wires running from my heart to the outside world was surreal.
I also worried about "pump head" — a cognitive fog that can follow surgery involving the heart-lung machine. It affects memory, concentration, language ability, and even personality. I'd read about it in Sandeep Jauhar's "Heart: A History" — it can "persist years after surgery and in many cases is probably irreversible," he wrote. My primary-care physician had also warned me that my brain might not work properly for weeks or even months after the surgery. Considering what I do for a living, that prospect alarmed me. But I was fortunate. My memory, attention, and sense of self remained intact. On the other hand, for weeks I experienced strange visual auras — the kind that usually precede a migraine but without the pain. My doctor was baffled. No one could say for sure if it was a delayed effect of anesthesia, the heart-lung machine, or simply my body's eccentric reaction to trauma.
The pain, at first, was unrelenting. Not just in my chest, which I had expected, but radiating through my upper back. For weeks, I was constantly being reminded of the violence that had been done to my body in the name of healing. It was agonizing to cough; even more so to sneeze.
And yet, I quickly began to recover. Within a day I had been moved out of intensive care; a day after that I was taking short walks in the hospital corridor; less than a week after entering the hospital, I was discharged. Once back home I figured out how to take a shower unassisted. I climbed a flight of stairs (slowly). I even made my way to the Starbucks around the block — though the first few times I tried it, I had to stop for periodic rests.
As I have learned from my reading, a typical human heart beats three billion times over a lifetime, pushing blood through 100,000 miles of vessels — a network so vast it would circle the globe if laid end to end. That mine could literally be stopped cold and started again, and a failing valve removed and replaced with a new one, is an astonishment. We take such surgery for granted now. But when I was born, the type of surgery I just underwent was still unknown. The first time an aortic valve from a human being was successfully replaced with one from an animal was in 1965, the year I entered second grade.
Jauhar writes that until the late 19th century, the heart was considered untouchable — not just medically but metaphorically. For millennia it was regarded as the seat of human emotion and feeling, and that perception lives on in our language: We "take heart," "speak from the heart," "have a change of heart," or "give our heart" to another. When Barney Clark was scheduled to receive the first permanent artificial heart in 1982, his wife anxiously asked doctors: "Will he still be able to love me?"
There is something intensely human about the vulnerability of the human heart. Even in an age when more than 3,000 cardiac operations are performed every day, we still think of it as sacred territory. Perhaps it is.
For me, heart surgery was more than just a medical event. It was a confrontation with mortality and a chance to marvel at what science and surgery have made possible — and what they still cannot fully explain. That I am here, writing this, with a new valve pulsing away in my chest, is a gift I do not minimize. Like Wiesel, I too am "overcome with a feeling of gratitude."
Cardiovascular disease remains the leading cause of death in America. As Jauhar notes, nearly one in four Americans will die from it, despite all our progress. But we have come far. In the 1950s, open-heart surgery had a 50 percent mortality rate. Now it's often less than 1 percent. And while cardiology may be reaching the limits of what it can achieve, it still affords the precious chance to extend life — and to reflect on its value.
Open-heart surgery didn't make me wiser. But it did bring home to me that the heart is not merely a pump. It is, in more ways than one, the center of our being. And mine, once broken, beats on.
* * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * *
What I Wrote Then
25 years ago on the op-ed page
From "The new blacklisters," May 25, 2000:
Once upon a time, activists on the left hated blacklists and loved free speech. They embraced the classic position attributed to Voltaire: I disagree with what you say, but I will defend to the death your right to say it. Gay-rights advocates especially appealed for tolerance. Live and let live, they said. To each his own. Be open-minded.
No more. "Tolerance" now means no tolerance for speakers whose opinions on homosexuality are politically incorrect. We don't like what Dr. Laura says; therefore, she may not say it.
* * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * *
The Last Line
"'I used to hate the water.'
'I can't imagine why.'" — Chief Martin Brody (played by Roy Scheider) and Matt Hooper (played by Richard Dreyfuss) in Jaws (1975).
* * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * *
Jeff Jacoby is a columnist for The Boston Globe.
-- ## --
Follow Jeff Jacoby on X (aka Twitter).
Discuss his columns on Facebook.
Want to read something different? Sign up for "Arguable," Jeff Jacoby's free weekly newsletter.